Brain / Spine AVM
What is a brain AVM?
‘AVM’ is an acronym for Arterio-Venous Malformation. This is a cluster of abnormal blood vessels in the brain or spine. Normally, arteries bring the blood to the brain under high pressure – they have thick walls. After supplying the brain with oxygen and nutrients, the blood then moves to the veins, where it drains away from the brain under low pressure. In an AVM, there is an abnormal connection between the two, and the arteries connect directly to the veins through a tangle of abnormal vessels.
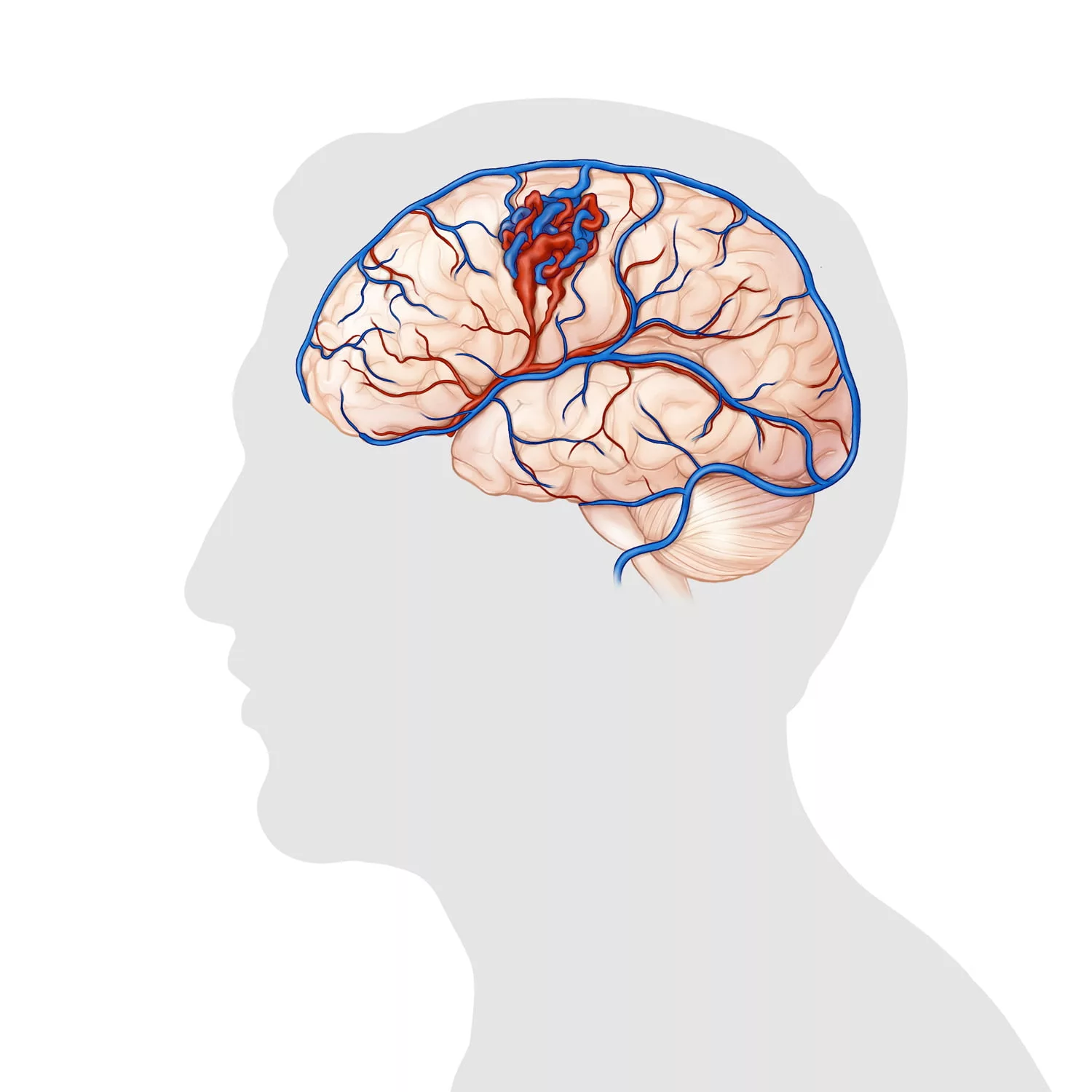
Brain AVM
What can it cause?
The main risk of an AVM is that of bleeding in the brain – a brain haemorrhage. This is because the poorly developed vessels within the AVM can rupture from the high-pressured blood from the artery. The risk of a bleed depends on the type of AVM, but generally speaking is between believed to be 2% per year. Certain types of AVM will have a higher bleeding risk than this.
Sometimes AVMs can also cause other symptoms. For example, some AVMs are found because of seizures. These happen because the AVM can irritate a part of the brain, and this can lead to a seizure. Other symptoms that an AVM can cause include headaches or neurological deficits resembling a stroke, as the AVM can drain blood away from other parts of the brain that need it. Many AVMs cause no symptoms at all, and are found when a scan is performed for another reason.
What causes it?
There is no single cause of an AVM. They cannot spread, and there is nothing you can do or change that will prevent one from occuring. There are some genetic causes – this is an area that we are researching, as we have a special interest in it. Some rare types of AVMs run in families. These are associated with a condition called Hereditary Haemorrhagic Telangiectasia, or Osler-Weber-Rendu Syndrome.
How is a brain AVM diagnosed?
They are most commonly found during an MRI or CT scan of the brain. If we are deciding whether to treat an AVM or not, or want to get a better look at it, we will often perform a test called a “cerebral angiogram”. This is an out-patient test. It is performed using local anaesthesia and sedation. It involves tracking a tiny tube, called a catheter, into the blood vessels in the neck. X-Rays of the brain are then taken while injecting x-ray dye or contrast. This allows us to get a much better look at the AVM.
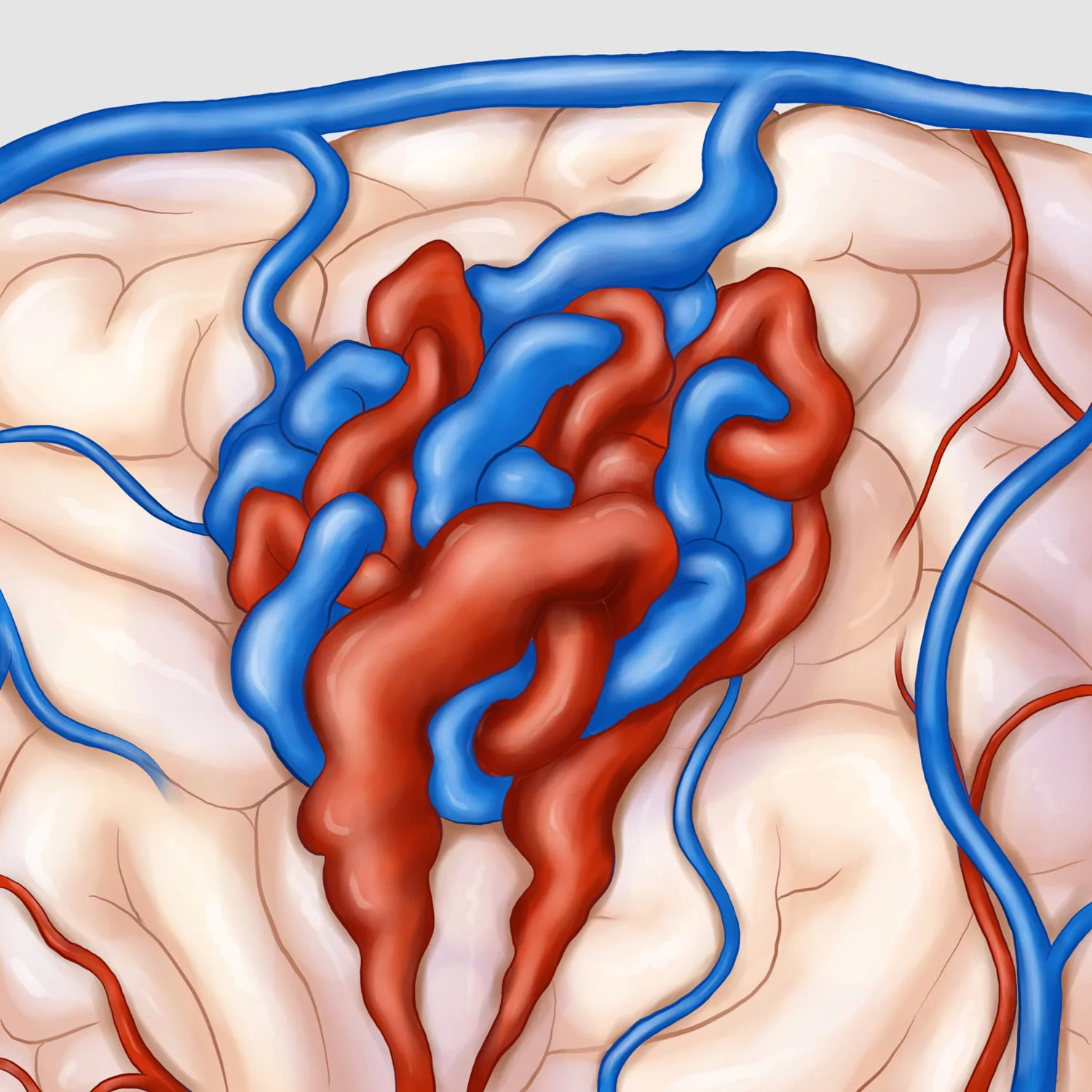
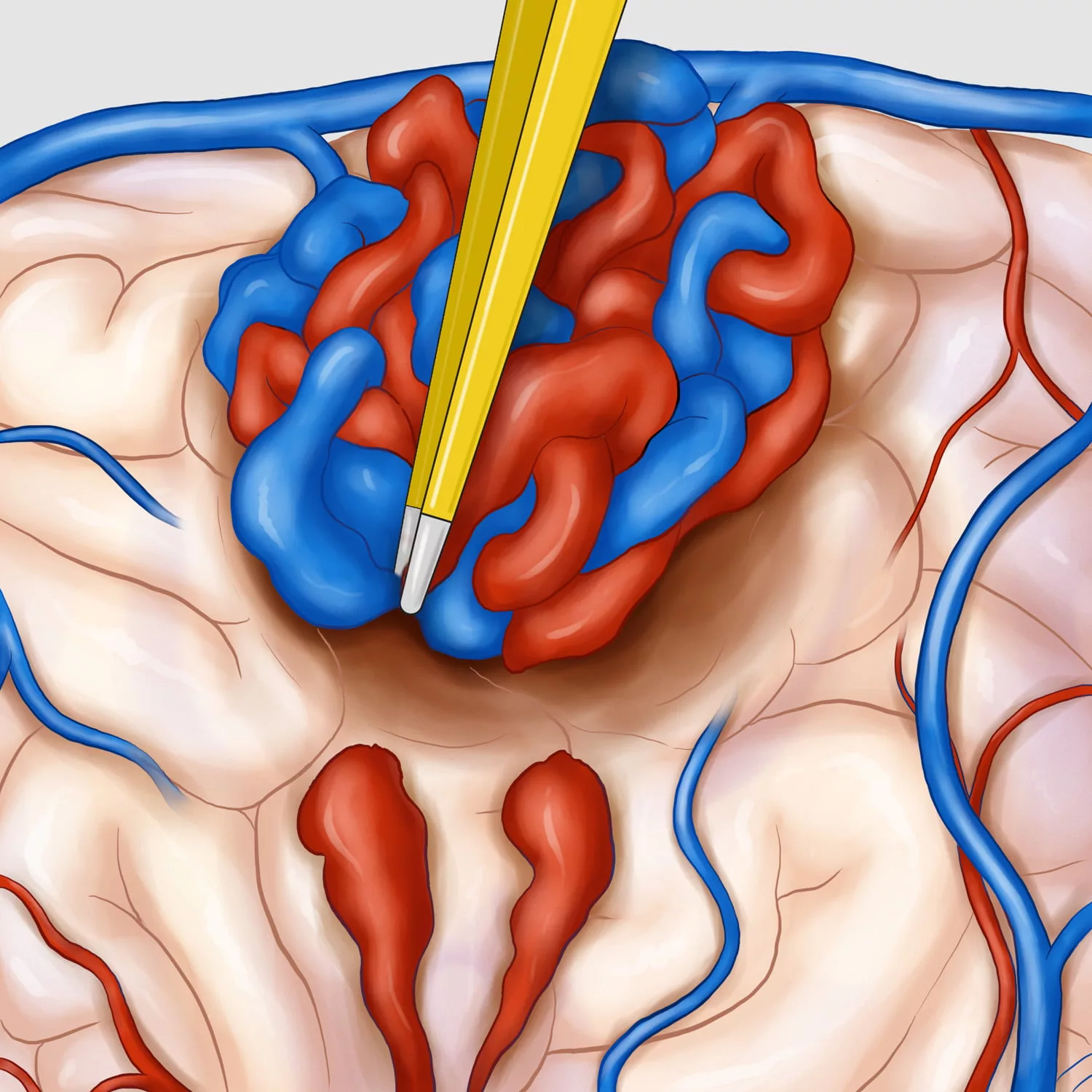
Brain AVM – Magnified View
When you are found to have an AVM, your doctor will refer you to our Neurovascular clinic at the Toronto Western Hospital. The Neurovascular Team has extensive experience in managing patients with brain AVMs. We discuss your symptoms (if you have any) and review your scans as a team to conclude on the best treatment for you and discuss our recommendation with you in the clinic.
Not every patient with an AVM needs treatment. Some of the AVMs have a higher risk of bleeding than others and we will often recommend treatment in these cases. When the risk of bleeding is deemed low, we may recommend follow-up and treatment of symptoms with medication.
What are the ways in which a brain AVM can be treated?
There are three main ways in which an AVM can be treated. Often we will combine two or more of these options when treating an AVM. It is important to realise that there is no single way to treat each AVM. This is why we think a team-approach is best, and why we sometimes will offer a combination of treatments. We will discuss all treatment possibilities with you, along with our team’s recommendation, when we review you in the AVM clinic. At our center we can offer all different types of treatment.
Radiosurgery/Gamma-Knife
This is a non-surgical treatment, which involves no general anaesthesia or overnight hospital stay. It is a precise way of using targeted radiation beams to close off blood vessels in the AVM. Each of these multiple radiation beams alone is not strong enough to damage the brain tissue on their own, but when they meet at the centre of the AVM they cause the blood vessels to thicken and scar. These blood vessels close off slowly over a few years, and so the full effects of the Gamma-Knife treatment often take a few years to fully work. Another angiogram is usually performed the morning of the procedure, to allow us to precisely plan where the beams have to go. The Gamma-Knife procedure itself often takes less than an hour, but the planning scans and other steps usually take up most of the day. Gamma-Knife is especially good for certain types of AVMs, such as those located deep in the brain where surgery might be more dangerous. It is also very effective for smaller AVMs. Following the Gamma-Knife procedure, we will follow the progress of the AVM with MRI scans over time.
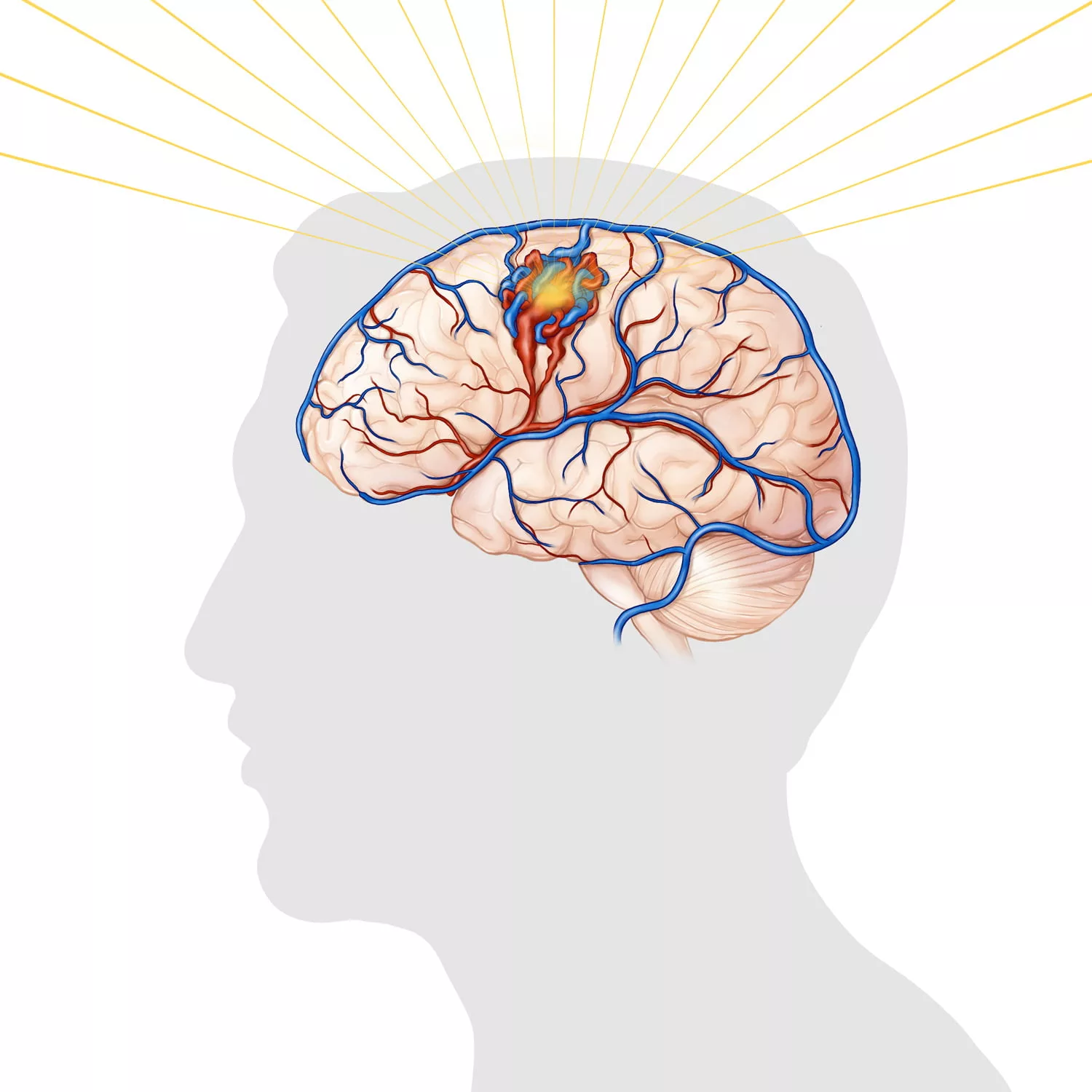
Radiosurgery / Gamma Knife
Surgery
This is performed while you are under general anaesthesia. Following an incision in the scalp, the neurosurgeon will use a high-powered microscope to carefully dissect and remove the AVM. Afterwards, you will usually be in hospital for a few days to recover. We will usually perform an angiogram or a CT scan to make sure the AVM is completely gone. After you go home, we will usually organise some follow-up scans a few weeks or months later. Following these, we will see you in the clinic.
Microsurgery
Microsurgery
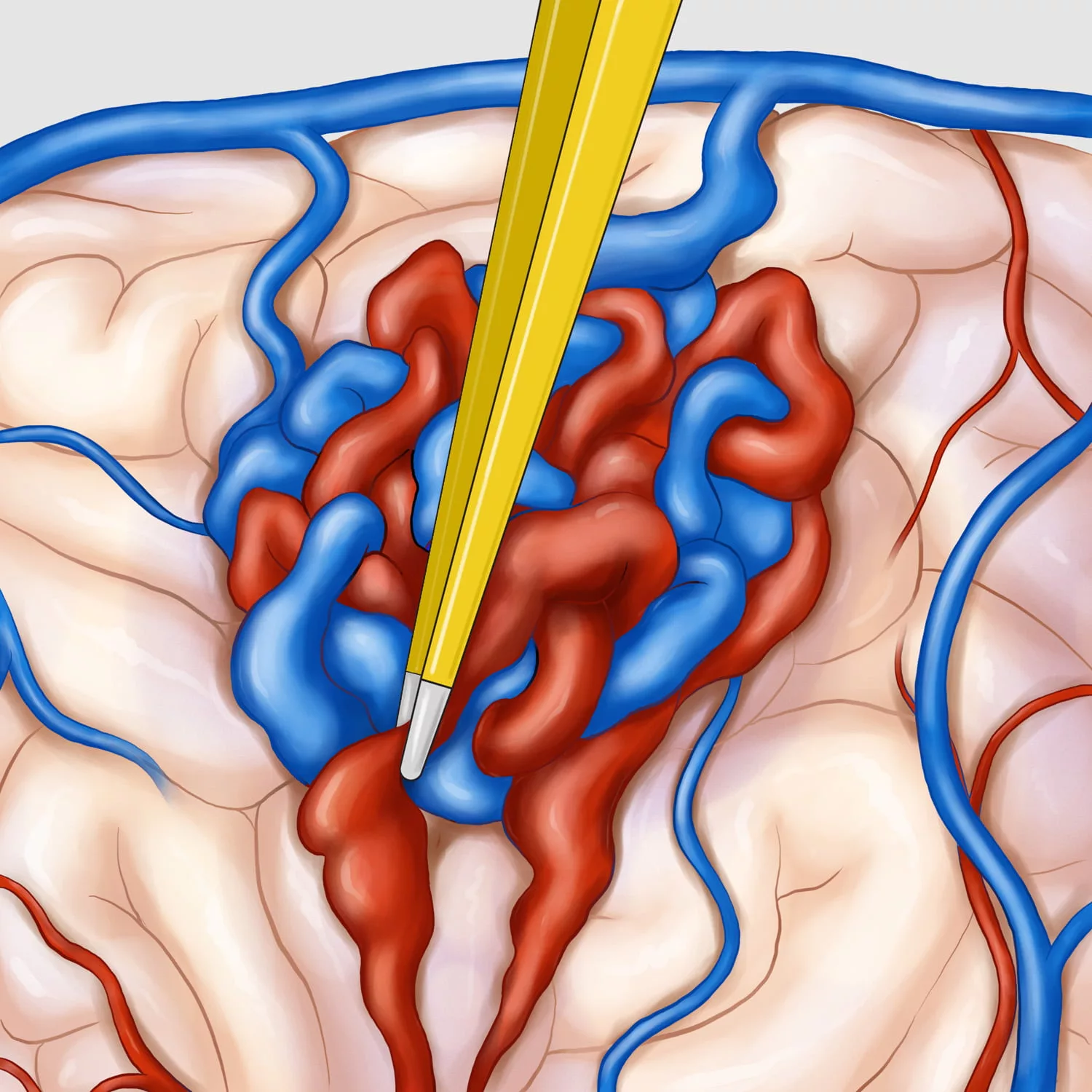
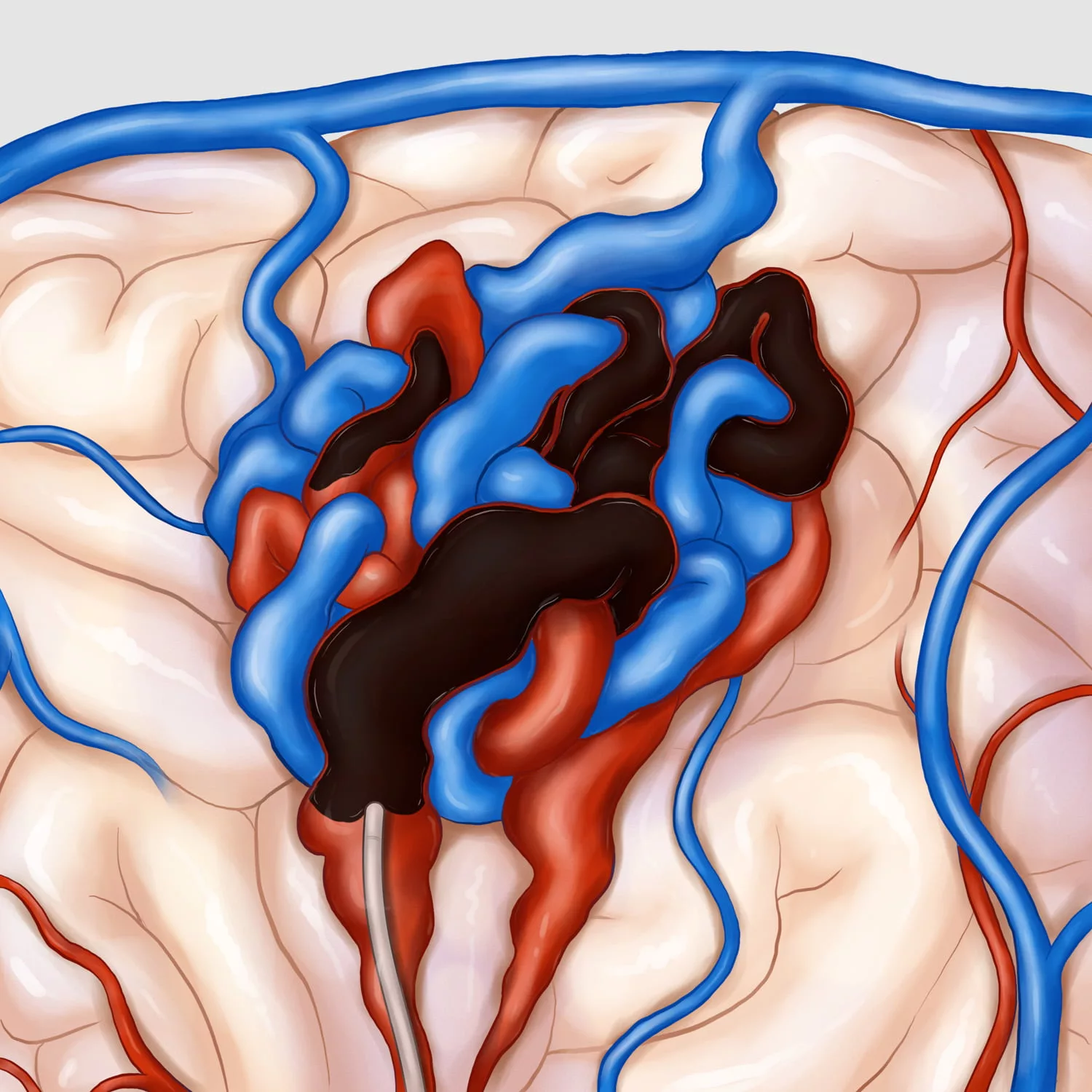
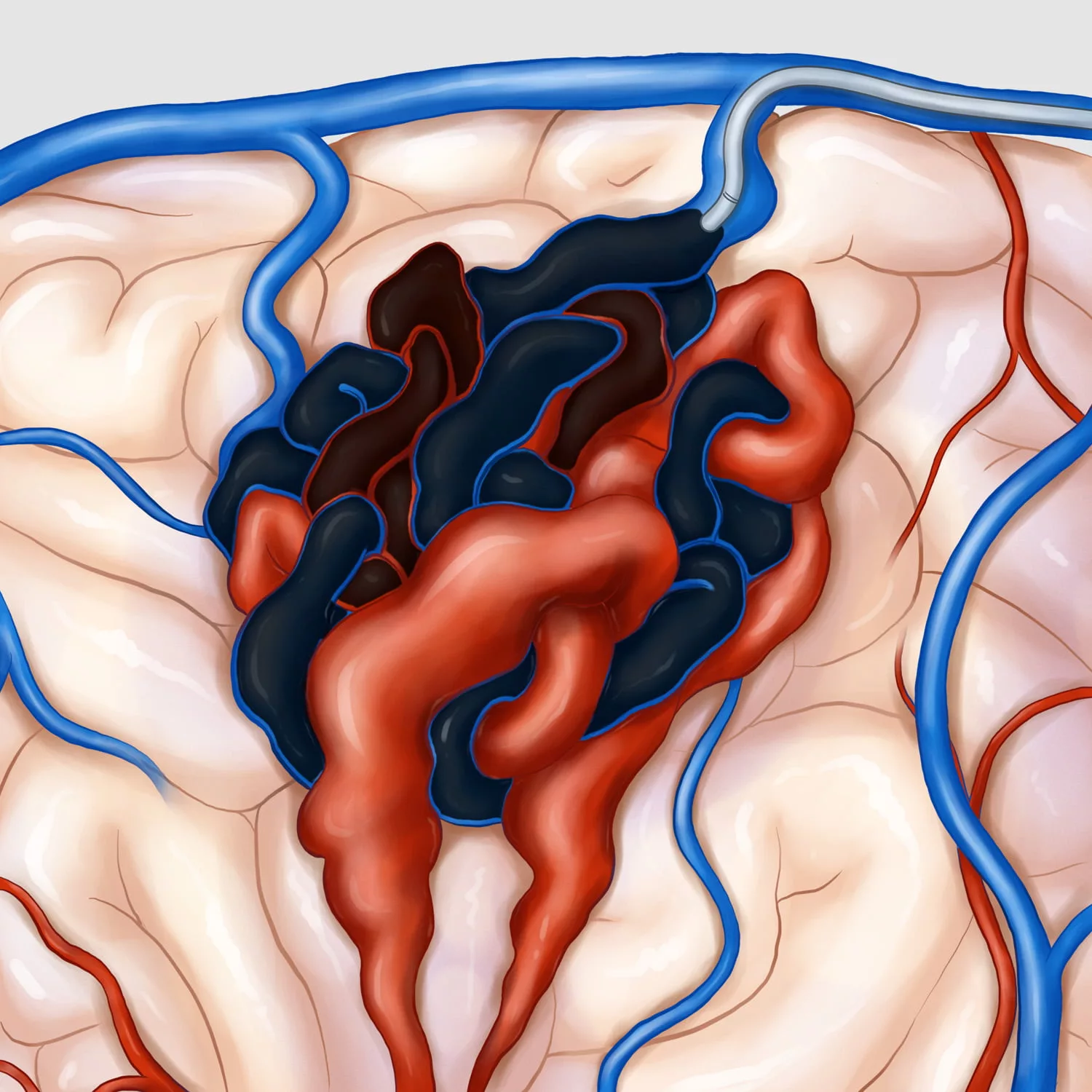
Embolisation
We can also treat some AVMs in the same way we do an angiogram. While you are under general anaesthesia, we can navigate small tubes or catheters into the blood vessels in your brain close to the AVM. We can then block off (or “embolise”) the arteries going to the AVM, to close them off. Sometimes we can do this first in order to reduce the size of an AVM to try and make it more suitable for radiosurgery or surgery at a later date. If we are treating an AVM by embolisation, we sometimes can treat it all at once, while sometimes we may need to treat it in several stages over a few months. After an embolisation you usually stay in hospital a night or two (if no further surgery has been planned). We will then discharge you, and usually see you in the clinic a few weeks-months later after some scans to make sure the AVM is gone.
Transarterial Embolisation
Transvenous Embolisation
Spinal AVM/dAVF
AVMs can also occur in the spinal cord. Another type of vascular lesion that can occur in or around the spinal cord or spinal canal is called a ‘fistula’. These can occur in the layers around the spinal cord, called the dura – these types are called spinal dural arteriovenous fistulas, or dAVFs.
These spinal AVMs/dAVFs can sometimes cause no symptoms and they can sometimes bleed. More often, however they cause congestion or edema of the spinal cord. This is because high-pressure arterial blood can ‘shunt’ into the low-pressure venous system which drains the spinal cord. The spinal cord can then get swollen, and this can lead to symptoms.
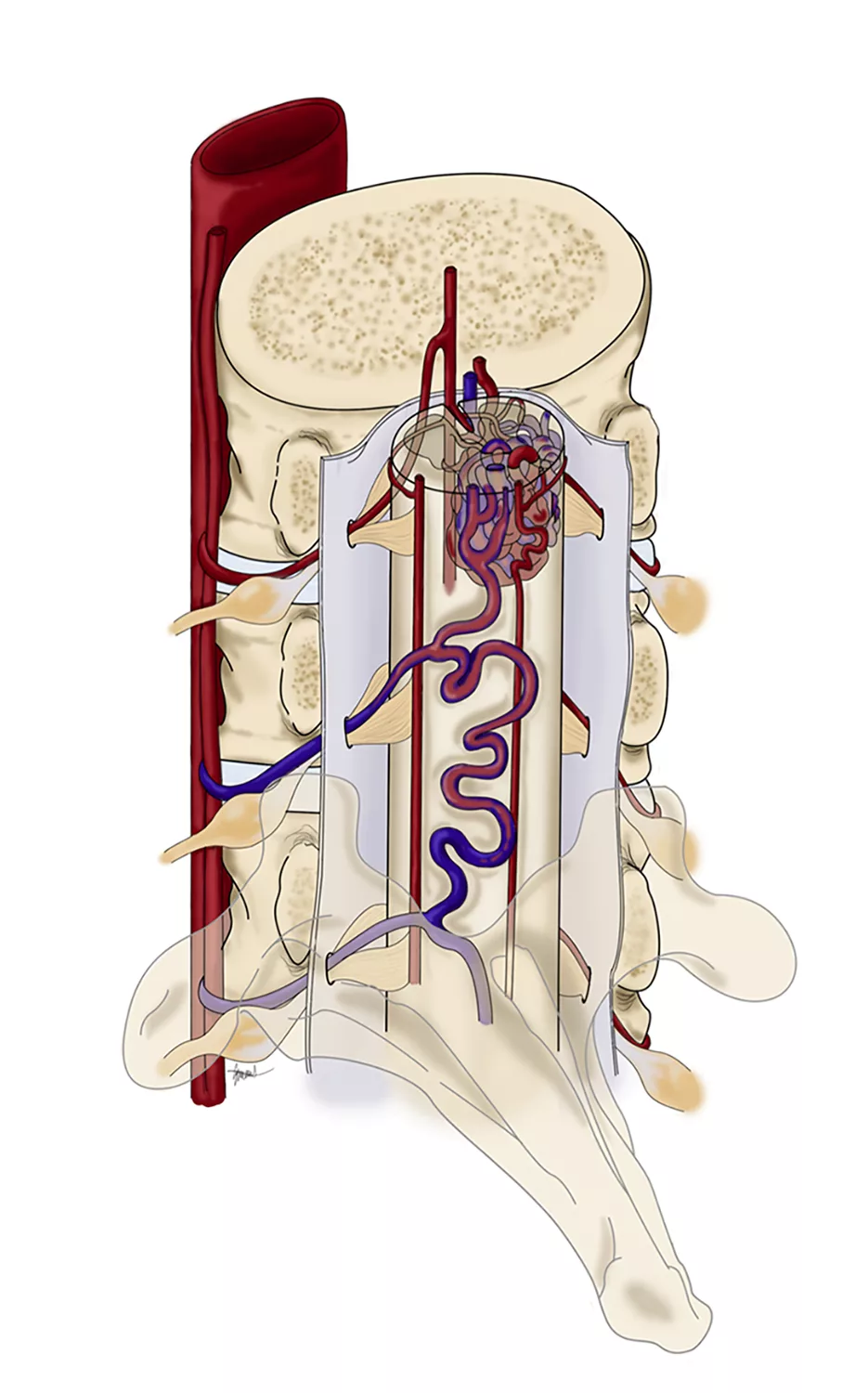
Spinal AVM
Spinal AVM
The symptoms that these lesions can cause depends on where in the spinal cord the swelling or the bleed is located. They can include weakness in the legs, problems with bowel or bladder function and sometimes pain.
There are various methods of managing these spinal vascular lesions. Some we simply treat conservatively, for example if they are causing no problems, or if we think they are not aggressive or will not cause problems in the future. If they are causing symptoms, the two main treatment methods are either open surgery or embolization. Open surgery is where a vascular neurosurgeon will disconnect the fistula or resect (remove) the AVM. Embolization involves navigating tiny tubes (catheters) in the blood vessels to reach the vascular abnormality and closing it off from the inside, by injecting various agents. We will discuss the various treatment strategies with the patient in the clinic.
Spinal dAVF
Spinal dAVF