Dural Arteriovenous Fistula (dAVF)
What is it?
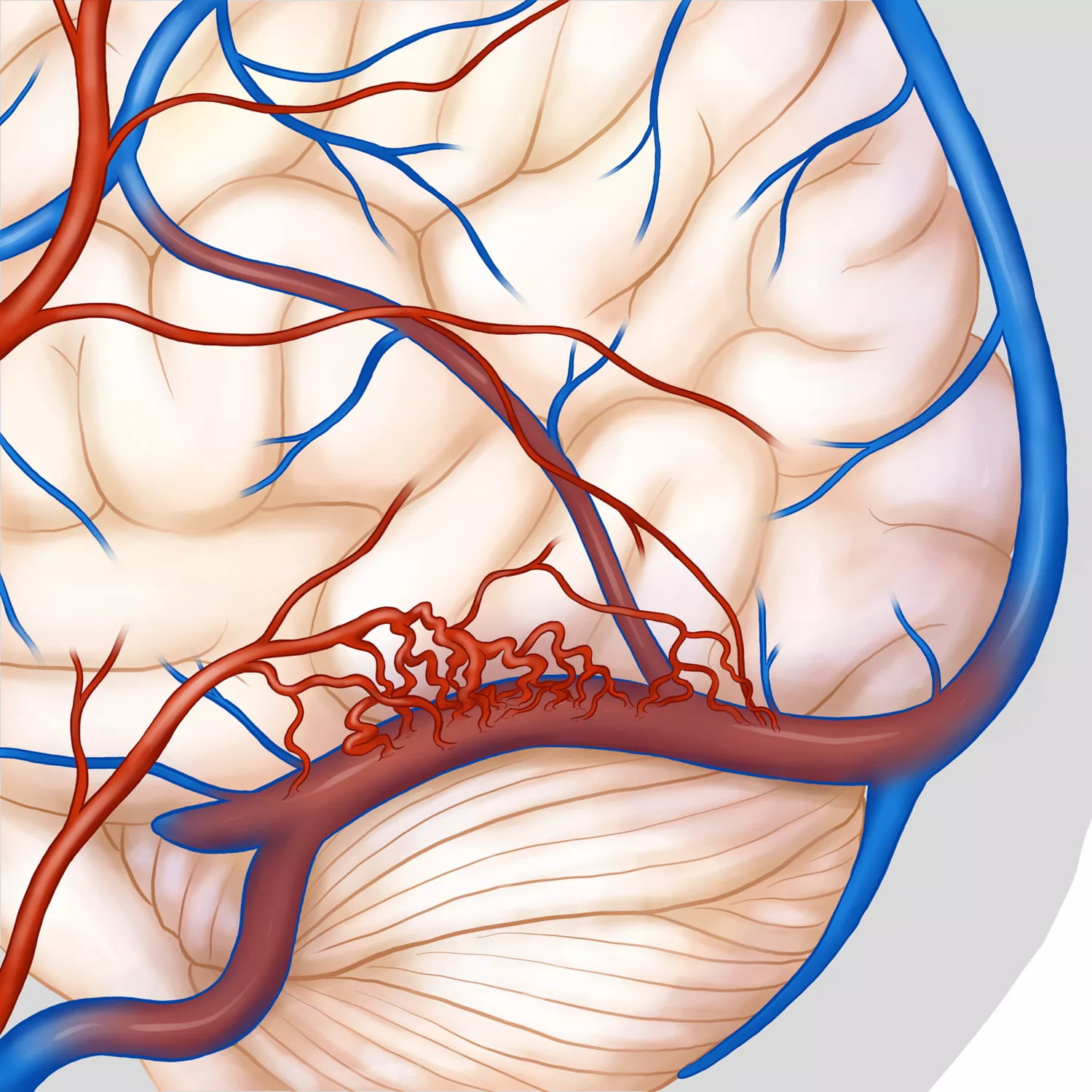
A dAVF is an abnormal connection between arteries and blood vessels in the brain. Normally arteries carry high-pressured blood which then supplies the brain, and the layers around the brain, which are called dura. Blood then drains into large draining veins around the brain, which are called the venous sinuses. These contain blood which is under low-pressure.
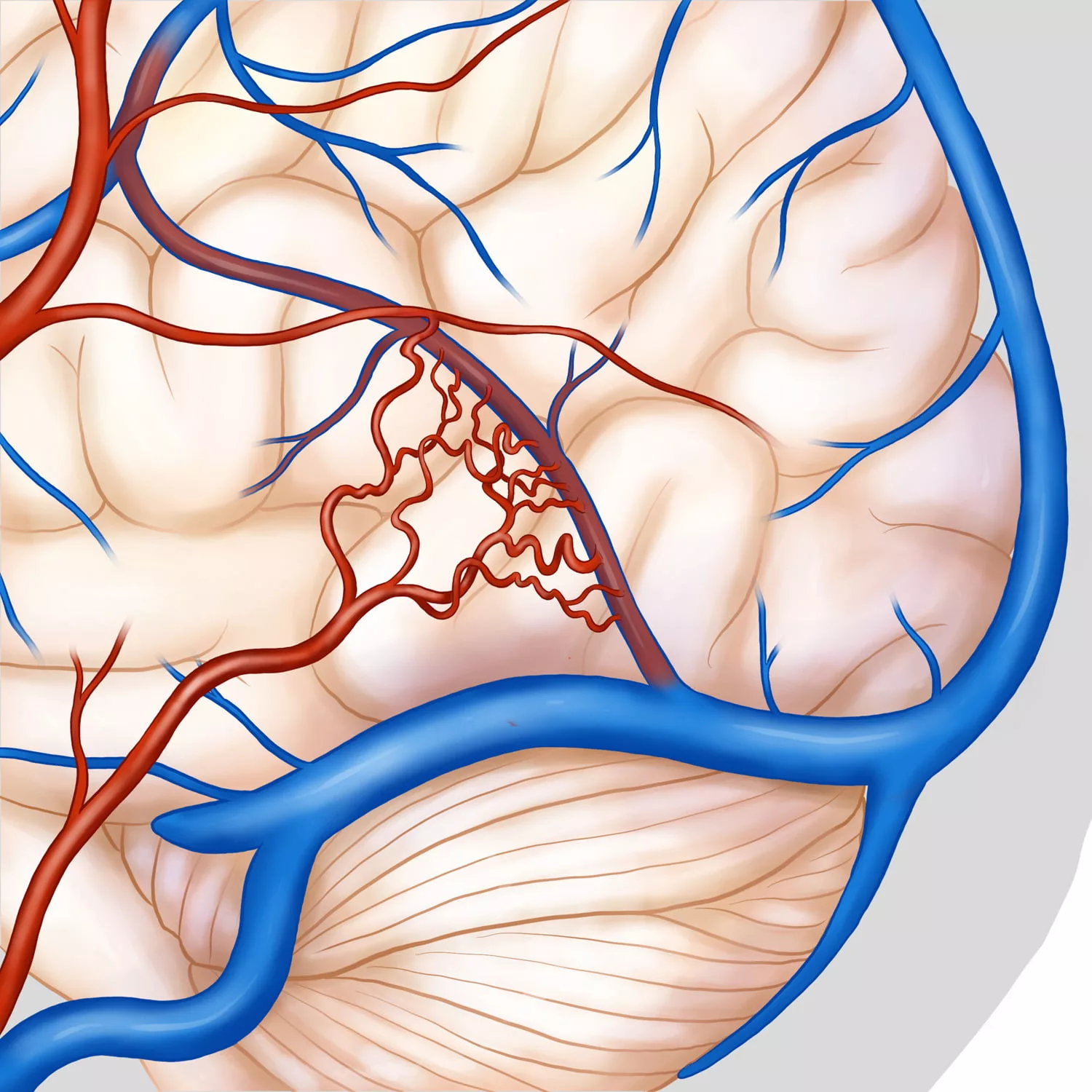
Sometimes, an abnormal connection can form between the arteries and the veins. This connection is called a fistula. It means that high-pressured blood from the arteries then drains into the low-pressure venous sinuses. This can happen and sometimes cause no symptoms at all. Ocasionally, it can cause back-pressure of blood into the brain. If this happens, the brain may not drain properly, and this can cause problems. The veins of the brain are not designed to deal with the high-pressure blood in an artery. This means that in some types of these dAVFs, you might be at risk of getting a haemorrhage, or a bleed in the brain.
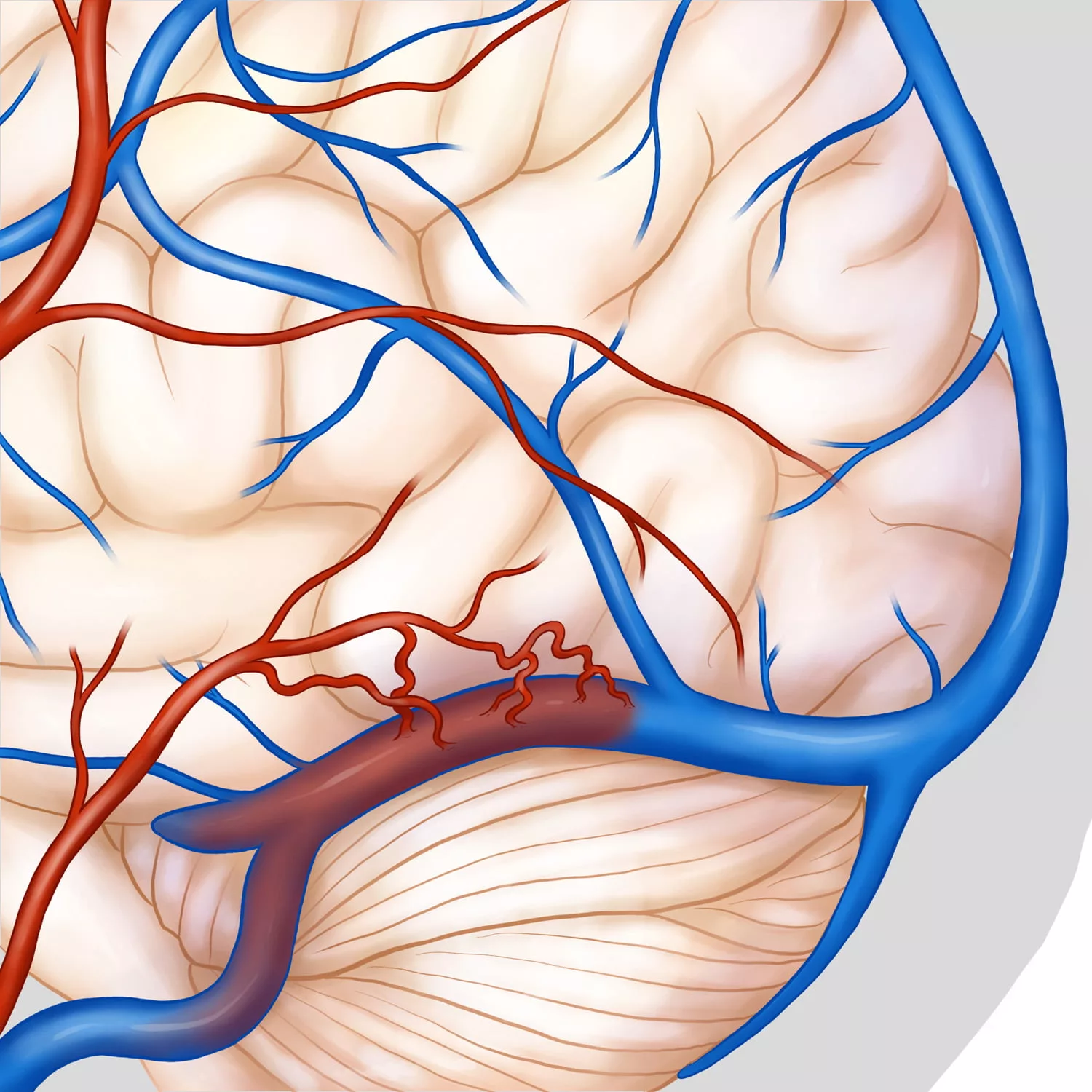
Normal arterial supply venous drainage of the dura.
How did I get it?
A lot of research has been performed to look at these dAVF, and nobody knows for certain how they are formed. The leading theory is that at some stage, a blood clot forms in the sinuses – the veins draining the brain. (This is like a clot forming in a deep vein in your leg on a long flight). This then causes “back-pressure” in the veins, and eventually this pressure is enough that a connection forms between these veins and the arteries which run very close by. Many research groups – including our own – have performed a lot of research on this condition.
How would I know I have one of these dAVFs?
As mentioned above, a dAVF can be completely asymptomatic. You might never know you have one, and sometimes they close off all on their own. Other people can get symptoms. These range from headache and dizziness to a severe “ringing” noise in the ears. This is called “pulsatile tinnitus”, because it often gets louder in time with the heartbeat or pulse, as the blood is pushed through the fistula. Some people can get a pressure sensation in their head. Others can get problems with drainage of the veins from their eyes – in severe cases this can affect your vision. More rarely, they can cause a blockage of the flow of fluid around the brain, a condition caused hydrocephalous. Very rarely, they have been known to cause a type of dementia.
How would I know if it ruptures?
A ruptured dAVF would result in a brain haemorrhage. The symptoms of this vary a little depending on where in the brain the bleed occurs, but they generally cause a severe headache, nausea, vomiting and sometimes even a coma.
Does every dAVF need to be treated?
No. As stated above, some of them will go away on their own over time as the body closes off the fistula between the artery and the vein. We grade the dAVF according to how much back pressure it puts on the draining veins coming from the brain. This grading system ranges from low-grade to high-grade. This grading system was designed to reflect the danger that the dAVF will bleed and cause a brain haemorrhage.
If the drainage from the vein is normal, it is considered a “low-grade” fistula. These may not need to be treated, and in some cases we will observe these with regular MRI scans. Sometimes, even if a dAVF is a low-grade one, we might decide to treat it after careful discussion with the patient. This is because sometimes the symptoms (especially “tinnitus”, the ringing in the ears we described earlier) can be so bad that it significantly affects the patient’s quality of life. But it is not uncommon for us to decide to observe these low-grade dAVFs.
High-grade dAVFs are at a higher risk of bleeding, as we discussed earlier. We usually recommend treatment for these, in order to decrease your risk of a brain haemorrhage over time.
You might ask why we do not just treat every dAVF? This is because the treatment carries some risk. The risk is usually quite small, depending on the type of treatment and the type of dAVF. The risk to the patient from the treatment is never zero, though. This is why we balance the need for treatment (and the risk of a bleed in the brain over the course of your life) against the risks of treatment. After we see you in the clinic, we will usually perform an out-patient test called a cerebral angiogram in order to get a better look at the fistula and it’s drainage pattern. We will have a long discussion with you in clinic regarding these risks if we decide to recommend treatment. In the end, it is always a joint decision between you, the patient, and our team.
If my symptoms go away suddenly, does that mean I am cured?
Not necessarily. Sometimes this means that indeed the fistula has closed off, and the high-pressure blood from the arteries is no longer being shunted into the veins around the brain. Sometimes however this can mean that the blood has found another drainage route from the brain. Occasionally, these means the the dAVF can change from a low-grade (safer) type to a high-grade (more dangerous) type. This is why it is very important that if you know you have a dAVF and your symptoms change significantly, you should arrange to come back and see us in our clinic urgently.
What are the ways in which a dAVF can be treated?
Endovascular Treatment
This is the most common way that we treat these dAVFs, and we have a lot of experience in treating dAVFs in this way. It is performed under general anaesthesia, and you will usually be admitted that morning. It involves us accessing the arteries and veins in your brain, usually through the groin. We can then navigate tiny tubes called “catheters” to the arteries and brains in the vein. We can then try and close off the fistula – the abnormal connection between the artery and the vein. There are a number of ways we can do this, but they all involve injecting something into the fistula (and the blood vessels beside it) in order to close it off. In this way, the arteries and the veins are disconnected from each other, and the dAVF is cured. We always keep you in hospital for at least one night after this procedure, and sometimes more. Following the treatment we will follow you up with MRI scans to make sure the dAVF has gone away.
Surgery
Surgery is also used for the treatment of dAVFs. This is especially true for some types that are very easy for the surgeon to get to. By making a small hole in the skull, the neurosurgeon can close off the connection between the artery and the vein. This is also performed under general anaesthesia, and you will usually be in hospital for a day or two afterwards. Again, we have a significant experience in treating dAVFs in this way.
Gamma-Knife/Radiosurgery
We can also treat dAVFs with radiosurgery, and some types are best suited to this approach. This means targeting hundreds of very weak x-ray beams on the connection between the artery and the vein. The beams are individually too weak to have any effect, but where they meet at their target their combined effect is very strong. They case the blood vessels which are abnormally connect to scar and close off. In this way, the fistula is closed off. This is performed as an out-patient procedure. You will usually need an angiogram – like the one you had done to investigate the dAVF to begin with. This is performed the morning of your Gamma-Knife procedure, and allows us to precisely target the area we need to treat. The treatment itself usually takes less than an hour. You have to wear a specially fitted mask to keep your head very still during the treatment. Gamma-Knife does not usually require that you stay in hospital afterwards, and you can usually go home the same day. Our group is also very experienced with using Gamma-Knife to treat dAVFs.
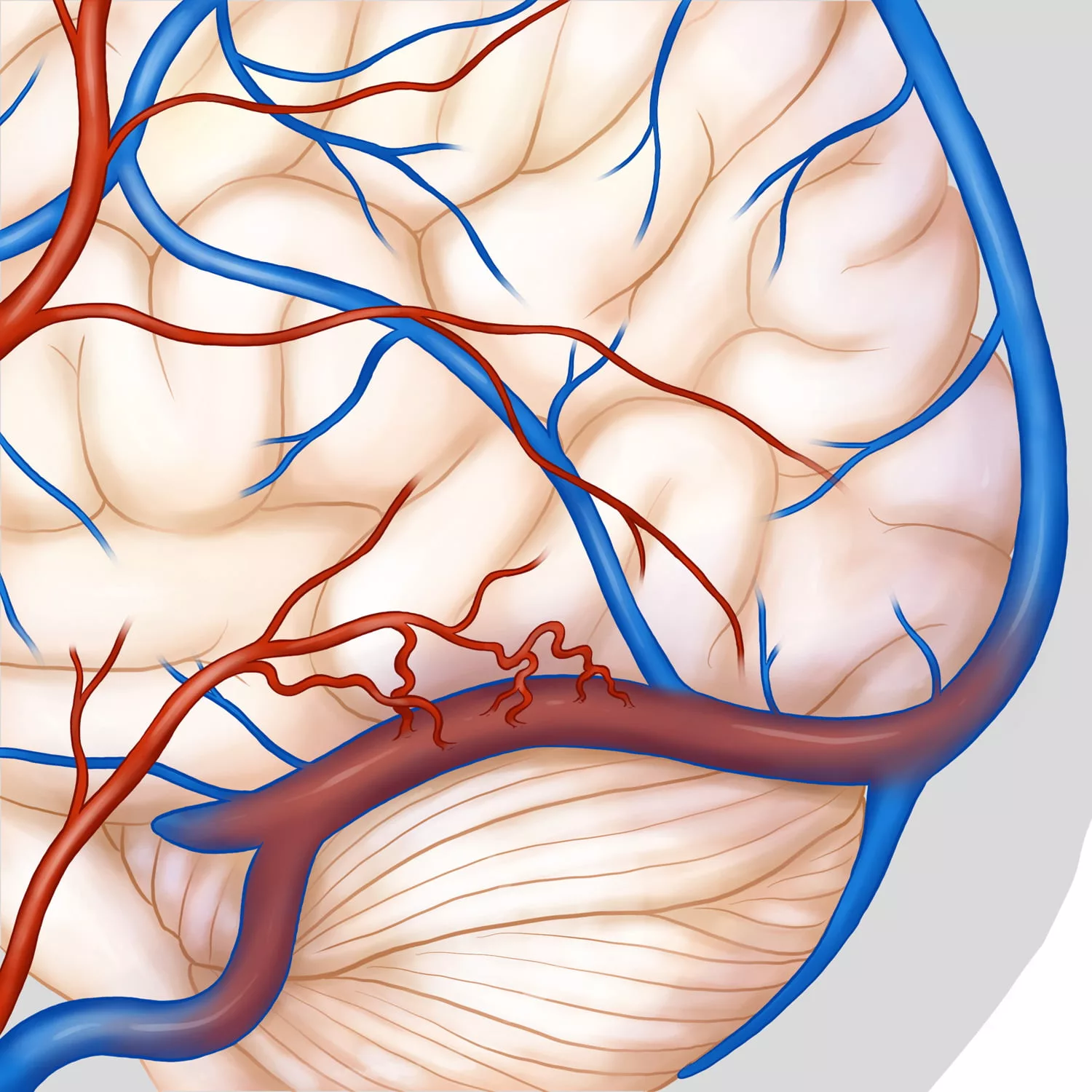
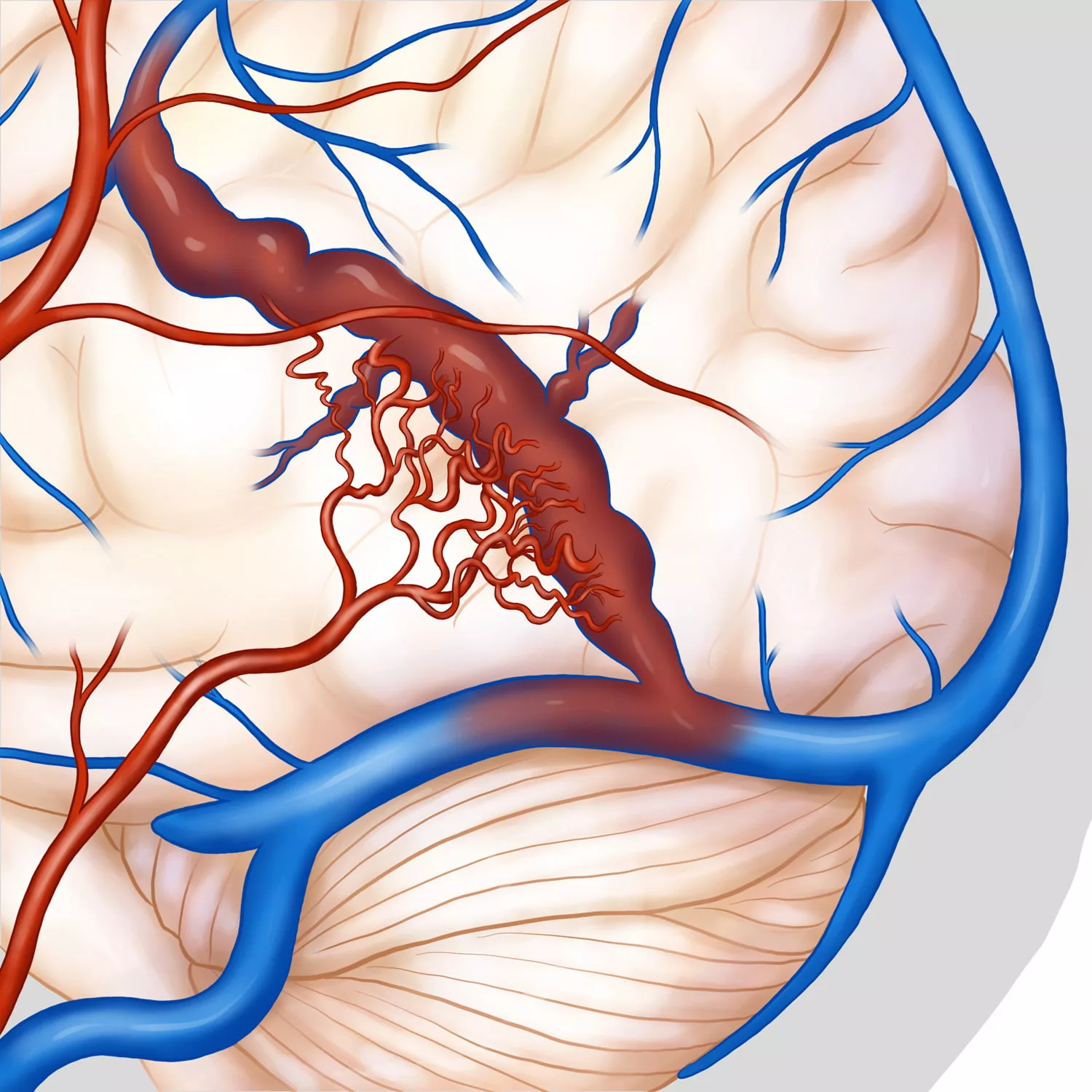
Showing progressive worsening – There is worsening reflux of blood in to the veins.
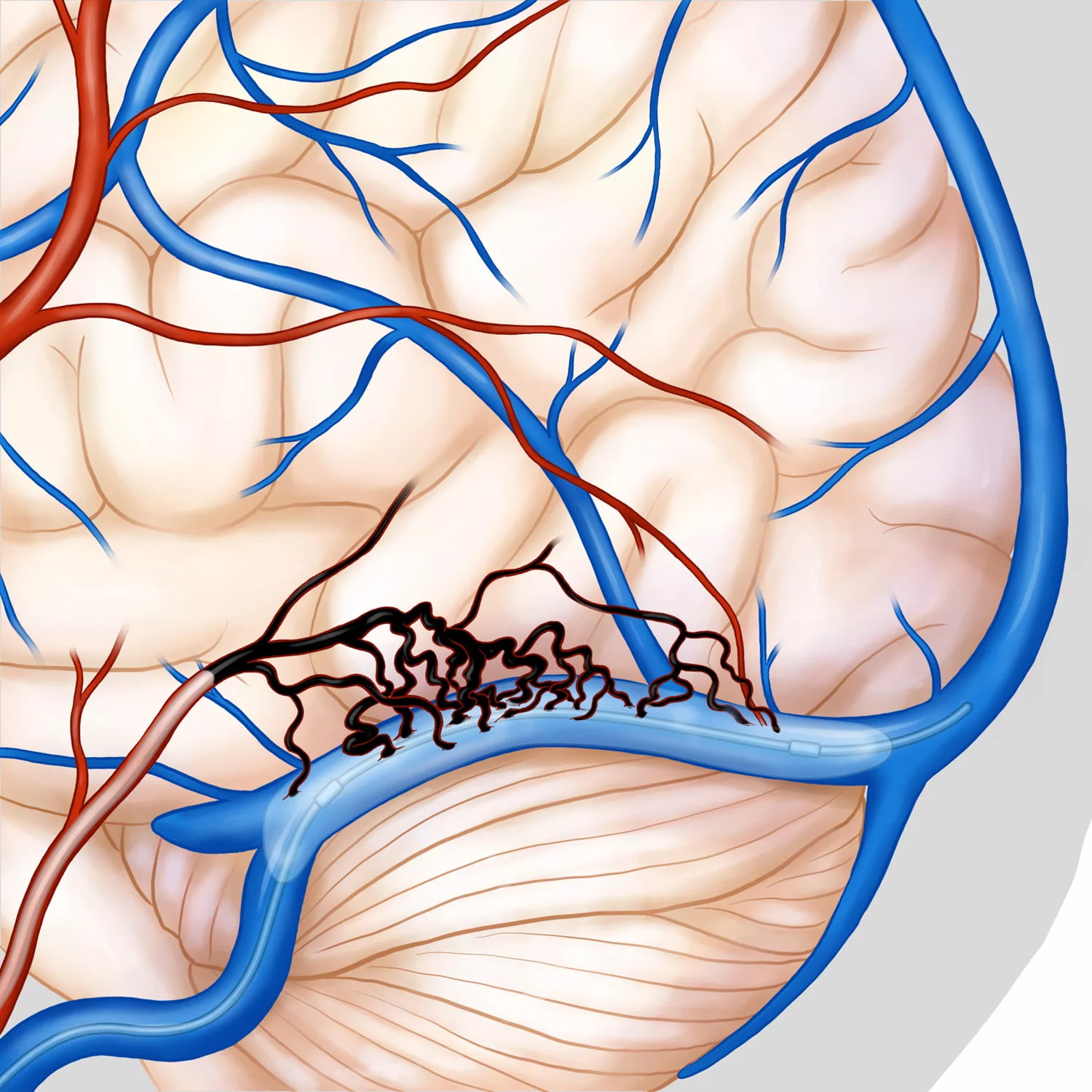
Transarterial Embolisation of Dural Fistula (dAVF) Onyx – A balloon has been placed in the transverse sinus in order to protect it.